


by Sherman J. Silber
completely revised and updated (2007)

VASECTOMY REVERSAL AND MICROSURGERY
I typically am called upon to reverse the vasectomy of men who have already had one, two, or even three previous failed attempts by other surgeons at vasectomy reversal. You need to understand why they failed and how we are able to perform a delicate operation repairing the fragile ductwork closer to the testicle (the epididymis) and thus, routinely restore fertility no matter how long ago the vasectomy may have been done.
The problem with cases like this is that pressure buildup from the vasectomy causes damage to the delicate ductwork closer to the testicle. When we bypass the epididymal damage, the sperm count returns to normal levels. We have performed many thousands of such successful operations on men whose first vasectomy reversal had failed despite what appeared to be an accurate reconnection of the vas. Therefore, most men with this problem now can once again father children, so long as the correct approach is taken, which is more complex than simply reconnecting (even with microsurgery) the severed vas.
Vasectomy Reversal Pitfalls
Unfortunately, there are many patients who receive poor microsurgical care by physicians who do not have the proper expertise and who commercialize vasectomy reversal for easy profit. So there are many traps to watch out for when choosing a doctor to perform your reversal.
For example, some doctors will offer a “money back guarantee,” but patients rarely get their money back after a failed procedure despite promises to the contrary. We have operated on many patients whose previous vasectomy reversal attempts at “money back guarantee centers” had failed, and none of these patients have ever gotten their money back. There was always some fine print wording that allowed the clinic to keep their money despite the “money back guarantee.”
In most so-called “centers,” the only procedure performed to reverse the vasectomy is “vasovasostomy” to try to reconnect the severed vas. However, in most cases there is also “epididymal” blockage (closer to the testicles) created by the pressure build-up after vasectomy. Thus, there is no chance for most cases of “vasovasostomy” to be a success, because there is also blockage in the more delicate duct closer to the testis, and this would have to be bypassed also with a very tricky-to-perform“vasoepididymostomy” [technical video] in order to have a successful result.
Another trap is that these less successful commercial operations are always performed at little outpatient centers or clinics, and not at a major hospital like St. Luke’s Hospital in St. Louis. Therefore, the patient is sent home, or to his hotel room, only a few hours after his operation. The natural consequence is often a huge amount of pain and swelling, and several miserable months of post- operative recovery. We think it is imperative for the patient to stay overnight for one night in the hospital, with drains in place and nurses changing the dressings, which prevents pain and swelling and results in a faster and much more pleasant post-operative recovery. When we “redo” a messed up “vasovasostomy” done elsewhere that had failed, despite it being a bigger operation to bypass all the scar tissue created by the previous failure, our patients are elated by how little pain and swelling they had to endure compared to their original failed reversal surgery in an outpatient office or clinic setting.
In fact, the only reason to do this operation in such an office or clinic setting is to save expense and make more money on the procedure. We do not condone this common practice. Furthermore, if cost is the important issue (and it is for many people), it is far less cost effective to have a “vasovasostomy” that fails, with significant pain and swelling afterwards, than to just do it right in the proper hospital setting the first time.
The next big trap is that clinics that cannot perform the delicate microsurgery required, will suggest you do sperm retrieval and IVF (in vitro fertilization) instead of vasectomy reversal. We have nothing against sperm retrieval and IVF, since it is our center at St. Luke’s Hospital that actually invented it in 1987, over 20 years ago. However, we invented it as a second choice approach for those in whom a reversal was not possible because of a complete absence of the vas deferens. Otherwise, it is so much nicer just to have one operation that restores your original fertility, without your wife having to go through months and months of painful injections involved in IVF, with a pregnancy rate lower than what you would achieve through natural intercourse once you have had a successful reversal.
Finally, it is important to realize that the testicles and the scrotum are a very private and sensitive area for most men. You don’t want to have a compromised procedure on that area of the body performed in the “procedure room” of an office based clinic, rather than in a proper operating room of a high quality hospital.
The “Simple” Microsurgical Operation to “Reconnect” the Vas Deferens
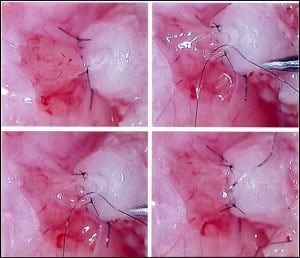
First lets discuss the “simple” approach, which works 20 percent of the time. Though it is easy to perform a vasectomy (it takes only five minutes in the doctor’s office), it is more difficult to reconnect it because of the microscopic size of the inner canal that carries the sperm. The outer diameter of the vas deferens is fairly thick, about one-eighth of an inch, and the tough outer muscular wall makes it feel like a copper wire through the scrotum. It is therefore an easy structure for the surgeon to identify and cut. But the diameter of the inner canal that carries the sperm is about one-seventieth to one-hundredth of an inch, or roughly the size of a pinpoint. This inner canal has a lining that is about three cells thick, approximately 1⁄2,000 of an inch. Vasectomy had always been considered a relatively permanent condition because of the obvious difficulty in surgically reconnecting such a delicate, tiny tube. With the microsurgical technique that we developed in the 1970s, this problem of reconnecting the vas deferens was solved, but the problem in getting high success rates goes far beyond this “simple” microsurgical reconnection. Just “reconnecting the vas” will give only a 20 percent success rate because pressure damage closer to the testicle, in the epididymis, prevents sperm from ever reaching the vasectomy site. Over 95 percent success rates can still be achieved with microsurgery to bypass epididymal damage, but this surgery is much more delicate than just “reconnecting the vas.” (see Figure 15.1) But for the moment let’s get back to the “simple” microsurgery for reconnecting the severed vas, since in some cases this is all that is needed. In order to achieve a nonobstructed reconnection, it is necessary to stitch accurately, in two layers, the delicate inner lining in a leakproof fashion using a thread invisible to the naked eye (see Figure 15.1). This surgery is performed under a microscope with very high magnification, using delicate instruments especially designed by me for this purpose [see technical video]. Many patients are told that too large a segment of vas has been removed to allow a successful reconnection. That is completely untrue. They are told that their vasectomy cannot be reversed simply because the doctor who originally performed the vasectomy took out a huge piece of the vas rather than just severing it. Actually the majority of urologists take out an unnecessarily large piece of vas when they perform a vasectomy, but this in no way reduces the chance of a successful reconnection. This is because men possess an enormous extra length of vas, far in excess of what is necessary for sperm to transit from the testicle into the ejaculate.
I remember operating on one man in 1987 who had had simply the most incredible vasectomy I’ve ever seen in my life. The surgeon who performed his vasectomy must have been in a terrible mood that day. More than four inches of vas had been removed on both sides. This meant that not only the man’s scrotal vas deferens was completely gone, but also that much of his abdominal vas deferens had been pulled out with it. It was really hard to believe. I’ve never seen another case quite that bad before or since. To reconnect that vas required a huge incision going all the way into the hernia region of the abdomen. Even so, we were able to sufficiently free up the remaining portion of the abdominal vas so that it could come down into the scrotum and thereby reestablish his fertility. So previous surgery, no matter how messy, with enormous scarring and segments of vas missing, should never be an impediment to obtaining a successful reversal of vasectomy in the proper surgical hands.
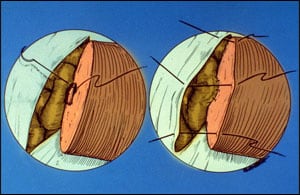
How Has Vasectomy Caused Blockage Closer to the Testicle?
After vasectomy, the testicle continues to produce fluid and sperm, which accumulates and dilates the entire sperm ductal system. Fluid and sperm thus accumulate in the epididymis, the tiny, delicate twenty-foot-long canal (coiled up into a length of only one inch) that carries sperm out of the testicle into the vas deferens. In this area the sperm ductwork is only 1⁄300 inch in diameter and the thickness of the wall of the epididymal duct is only 1⁄1,000 inch. This buildup of pressure is usually not felt by the patient because the duct is so tiny.
Eventually, the pressure builds up to a point where rupture or clogging occurs in the epididymis. This is the major culprit in restoring the man’s fertility. It is what prevents patients from recovering normal fertility despite what might be a proper reconnection of the vas. The good news is that with extremely refined microsurgical techniques, the damage in this area can be repaired or bypassed, and the success rate for reversal of vasectomy can still be quite good.
Length of Time Since Vasectomy
We originally demonstrated in 1977 that the longer the period of time since vasectomy, the worse the chance for successful reversal (despite an anatomically perfect reconnection of the vas). In 1978, we discovered the cause of the problem. The answer of course was that the pressure buildup caused obstruction in the epididymal ductwork between the testicle and the vasectomy site. The longer the period of time since the vasectomy the more fluid and the more pressure buildup. Thus there is a greater likelihood for epididymal damage.
To solve this problem we developed a more intricate microsurgical operation in which we could locate the points of epididymal blockage where normal sperm were present, and bypass them. So no matter how long the time since your vasectomy, we can have very high success, we just have to bypass the epidydimal blowouts. This is not just a simple “reconnection” of the vas.
How Is the Epididymal Blockage Bypassed?
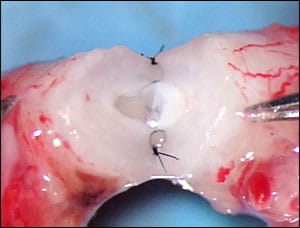
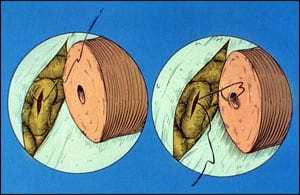
Under the operating microscope, we can microsurgically cut into the epididymal tubule moving closer and closer to the testicle until there is suddenly a brisk outpouring of huge quantities of sperm under high pressure (see Figure 15.3). The epididymal tubule is so fragile (the epididymal wall is 1⁄1,000 of an inch) that it must be sewn to the inner lining of the vas with thread that is virtually invisible to the naked eye. An absolutely perfect connection of that inner lining of the vas to the opening in the epididymal tubule is essential. As Figures 15.4 and 15.5 illustrate, there are two equally good ways to do this, “end-to-end” or “end-to-side.” If a sloppily performed attempt at reconnection is made, however, sperm will just leak out and result in scarring and either partial or total blockage. So this extremely difficult procedure must be performed perfectly.
ICSI with Retrieved Sperm
The technique for aspirating sperm from the male, and using that sperm for ICSI and IVF in the female, was actually invented by our group. This procedure involves direct aspiration of sperm from the husband combined with the injection of a single, weak or non-moving sperm into the cytoplasm of each of the wife’s eggs. We routinely perform this procedure for patients who have congenital absence of the vas, or for those in whom there is no possibility of surgical repair.
However, for anyone who has had a vasectomy, or even one or more previous failed vasectomy reversals, the simplest, most cost-effective approach, would still be to reconnect your ducts microsurgically. This involves no greater surgical discomfort than sperm aspiration and gives over a 95 percent chance for a successful return of fertility. It is certainly more cost effective and simpler to have a vasectomy reversal than going through multiple cycles of IVF and sperm retrieval.
REVERSAL OF TUBAL LIGATION
Female sterilization is the most popular method of birth control today for married women in their mid-thirties who have had all the children they want. But it need not be a permanent procedure. Tubal ligation is a simple, popular outpatient surgical procedure, but reversing it requires very specialized microsurgical skill. Sterilization by tubal ligation is most commonly chosen by women who are over thirty years of age, married, have several children, and don’t want any more. Women who are sterilized under the age of thirty usually come to regret it. Even women who have as many as three or four children before age thirty are very likely to want more. Furthermore, women who are unhappily married at the time of their sterilization are very likely to regret the procedure after they get divorced and remarried. Clearly, the women most likely to regret being sterilized are those who have the procedure performed under the age of thirty, who are now in an unhappy marriage, or who had had the procedure performed within one year of having their last child.
Methods of Blocking the Tubes
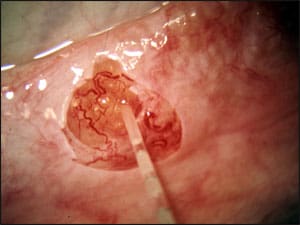
Microsurgically aspirating sperm from the epididymis moving closer and closer to the testicle until there is suddenly a brisk outpouring of huge quantities of sperm under high pressure.
Whether by minilap or by laparoscopy, there are four basic methods for occluding the tube. The classic method is to use a piece of surgical thread to tie off a loop of tube and cut out the section between the tie. A second approach is fimbriectomy, in which the entire fimbriated end of the tube is removed. This is a rarely used and terrible approach that makes the sterilization irreversible. As long as the fimbriated end is not removed, the tubal ligation can be reversed. There are several methods for occluding the tube through the laparoscope. The most common method is simply to “burn” the tubes with an electrocoagulating current transmitted through a special forceps. It has been feared that this burning (cautery) might make the sterilization irreversible by destroying the uterine side of the tube. However, even these “difficult” cases can be reversed successfully with proper microsurgical technique, which I will explain later in the chapter. The remaining laparoscopic methods involve physical occlusion of the tube rather than cautery. The Hulka clip (named after the gynecologist who invented it) reliably occludes the tube and damages only the tiniest portion. The Fallope ring is a small Silastic band with a special applicator that cinches around a doubled-up loop of the midportion of the tube. The Fallope ring also damages only a small portion of the tube, is easy to apply, and probably is the most commonly used of the easily reversible methods of tubal occlusion (see Figs. 15.6 and 15.7). Every method of occlusion must destroy some small segment of tube, which then scars down. As long as the fimbriated end of the tube is intact and as long as less than two thirds of the tube is destroyed, microsurgery can restore fertility back to what it would have been if the woman had never been sterilized. Simple, minimally destructive occlusion of the narrow isthmus region of the tube makes the most easily reversible sterilization, but that is not a requirement for reversibility.
Reversal of Tubal Sterilization
First delicate suture to connect the tiny epididymis tubule to the inner canal of the vas, end to side.
Jennie was a twenty-seven-year-old housewife with a boy age three and a girl age six. She had her tubal ligation performed laparoscopically after the boy was about six months old, and she was relatively sure that he was healthy and growing normally. The doctor doing the sterilization wanted to make sure there was no unwanted pregnancy because this couple did not think they could afford any more children. So he burned the tubes with bipolar cautery all the way down to the uterus. Three years later the little boy was riding with his father on a tractor on a calm, beautiful Sunday afternoon. He unexpectedly jumped off, and the big wheel ran right over him. He was dead instantly, and Jennie longed to have another child but was told that her tubes were just too badly burned to be repaired. Fortunately for her, we were able to reconnect the tubes to the microscopic openings coming out of the uterus (see Figure 15.8). So, despite the difficulty, if less than two thirds of the tube is destroyed, tubal sterilization can still be reversed. Jennie has had two more children since then and has no intention of ever being sterilized again. Jan had three children and a happy marriage, and she had decided to have a sterilization three years before seeing me. Two years after the sterilization, Jan and her husband, Roger, knew they wanted a larger family and could afford more children. They had done such a good job of raising the three they already had that I felt quite sure there was room for more children if they wanted them. Yet when their local gynecologist, a well-known fertility expert, looked at Jan’s tubes through the laparoscope to decide whether a reversal procedure could be performed, he sadly concluded that nothing could be done. The tubes had been “too badly damaged” by the original sterilization procedure. When we looked at his report, we realized that the fimbriae were not damaged, and although the ampullae were short, they certainly were long enough to nourish the egg. What had concerned her gynecologist was what looked like a technically difficult operation because of a unipolar cautery sterilization that had burned the tubes all the way down to the uterus. The opening to the uterus is so tiny that such an operation requires a great deal of microsurgical skill (see Figure 15.8). But still, virtually all such cases can be reconnected, and I knew there was enough healthy tubal length for pregnancy to occur. So Jan came to St. Louis to have her tubal reversal. Jan and Roger now have two more children.
How the Type of Sterilization Affects the Technique for Reversal
Final sutures for connecting the vas to the epididymal tubule, bypassing all secondary blockages.
In the past, unipolar cauterization (burning) through the laparoscope has been the most common method of sterilization. This usually results in destruction of a fairly large segment of tube. Fortunately, the burn always seems to spread from the grasping forceps to the uterus, sparing the end of the tube leading toward the fimbria. It burns all of the isthmus right down to the uterus, and some of the ampulla. Thus, it is technically the most difficult type of sterilization to reverse. But because tubal length is often quite adequate, we still have an extremely high success rate with reversing this type of sterilization. But the technical difficulty of such a procedure usually overwhelms doctors who are not extremely experienced in microsurgery. For that reason, unipolar cautery is not an easily reversible sterilization. The type of reconnection required after unipolar cautery is called ampullary-cornual, meaning that the large-diameter ampulla has to be reconnected to the tiny cornual opening of the uterus. To perform such an operation requires either making a tiny opening in the scarred ampulla so that openings of the same microscopic size can be connected, or cutting out the scar and tailoring this enlarged opening down to the tiny one-seventieth of an inch diameter that will allow it to match up with the tiny one-seventieth of an inch opening of the cornual end (see Figure 15.9). Bipolar cauterization (also performed through the laparoscope) allows the current to go down one tong of the forceps across the tissue to the other tong and never spreads anywhere but between those two points. Thus, the tube is burned wherever it happens to be grasped, and the burn does not spread in either direction. This type of cautery will damage very little tube, and if the tube is grasped in the narrow isthmus region, should result in the blocked ends of the tube being of relatively equal size and not very difficult to reconnect with microsurgery. The only catch here is that many doctors are so afraid that this bipolar cautery does not burn the tube adequately that they may burn the tube in several different places. This does not mean the sterilization is irreversible, only that more complex surgical techniques are required for the reversal. The Fallope ring is a tiny Silastic band that looks like a very thick, round rubber band with an internal diameter of about one eighth of an inch. It comes loaded on a device that grasps the fallopian tube through the laparoscope or minilap and then pulls a loop of it up through the ring. Because the ring is so tight, the loop of fallopian tube loses its blood supply and disappears into scar tissue over the course of several weeks. Usually this procedure destroys very little tube, and it virtually always leaves enough tubal length for subsequent reversibility. Like the bipolar cautery, it usually doesn’t damage the tube all the way down to the uterus, so a difficult cornual reconnection is not required. The only technical problem sometimes created by the Fallope ring and the classic tubal ligation is that often an area of isthmus and ampulla, rather than just isthmus alone, is destroyed. This means that to reconnect the tube requires surgically uniting the relatively large diameter of the ampulla to the somewhat smaller diameter of the isthmus (see Figure 15.9). The easiest surgical reconnection is with lumens of the same diameter, and that is where the Hulka clip comes in. The Hulka clip never damages more than one fourth of an inch of tube. So if it is applied to the isthmus region, the reversal operation would simply involve reconnecting isthmus to isthmus, lumens of the same diameter.
What Factors Affect Successful Sterilization Reversal?
Tubal ligation and healed tubal ligation.
If we look at the success rates in various groups of patients on whom we performed a sterilization reversal, we get a clear picture of what factors affect reversibility. Virtually all our reversal patients have had a good connection,with perfectly open and normal tubes postoperatively. But despite near-perfect surgical results, not all our patients have gotten pregnant after reversal of tubal sterilization. Looking at the various categories of these patients helps us understand what makes the sterilization reversible and not reversible after a proper microsurgical reconnection.
The observations recorded for each patient were the age of the husband; the age of the wife; the sperm count of the husband; the number of previous children (if any); the duration of time since the sterilization was originally performed; the type of sterilization procedure performed (whether through laparoscopy, laparotomy, or minilaparotomy); whether unipolar or bipolar cautery, Fallope ring, Hulka clip, or ligation was used; the area of the tube that was destroyed; the areas of the tube that had to be reconnected; and, finally, the total length of tube remaining after the reconnection was achieved. Furthermore, we observed the character of the anatomic appearance of the ovaries, the quality of the menstrual cycle before and after the reversal surgery, and the amount of general scarring (adhesions) in the pelvis.
Hulka (spring) clip and Fallope ring.
We hoped to find the answer to three specific questions: (1) What type of sterilization procedure is easiest to reconnect surgically? (2) Are there any types of sterilization procedures that are impossible to reconnect surgically? (3) Assuming a good reconnection is achieved, would anything else about the way the sterilization was originally performed stand in the way of getting pregnant now that the tubes were properly reconnected?
Microsurgical suturing of fallopian tube.
We found that the only things that affected whether these women got pregnant after sterilization reversal surgery were the length of tube on the longer side and her age.None of the other myriad factors we carefully and assiduously studied made any difference.As long as there was a fimbria left to pick up the egg, there was nothing else about the sterilization procedure that prevented pregnancy other than the length of tube that was left after the reconnection. In fact, the pregnancy rate over time was no different from what would occur based on age in a normal population of women.
The type of sterilization, whether through a laparoscope or a minilap, made no difference. Whether the tube was blocked by unipolar cautery, bipolar cautery, Fallope ring, Hulka clip, or ligation made no difference. The pregnancy rate was diminished only if the tube was less than one and a half inches long when the procedure was completed.
How Difficult Is Tubal Reversal Surgery for the Patient?
In the mid-1970s, when we performed the very first tubal microsurgery in the U.S., it involved a major abdominal incision, a week in the hospital, and a six week postoperative recovery. The actual microsurgery was delicate even then and posed no threat to the patient. It was just the surgical exposure that made it a very big operation. So whether or not to undergo the surgery was a formidable decision for any woman who was rethinking having more children.
Today, however, even the most intricate tubal microsurgery can be performed by us as an outpatient procedure through a very small incision. The patient only needs to be out of work for a week and essentially needs no postoperative care. The surgery requires only a one-inch minilap incision just below the pubic hairline. A very unobtrusive plastic retractor allows us to get a microscopic view of any area we need to reconstruct through such an incision.We can even do an ovary transplant using this approach, and send the patient home on the same day or the next morning. Therefore, it is easier and more cost-effective for a woman to have her tubal ligation reversed than to undergo an IVF procedure. There is very little pain or inconvenience resulting from our microsurgery.
We have seen many requests for reversal of sterilization by women whose husbands also need vasectomy reversal. If we weren’t so certain about the return to normal fertility of women who have an adequate length of tube left, we would have difficulty suggesting that both the husband and the wife undergo surgery to try to have children.
Wanda and Bert were the first such couple I treated. Each had several children from previous marriages. They were now blissfully married to each other in a happy, stable relationship, and both they and their present children wanted them to have more kids. Wanda was told there was no hope for reversing her sterilization because it had been performed with unipolar cauterization with too much tubal destruction.As in all cases of female sterilization reversal, only two issues mattered: Could we technically accomplish a surgical reconnection? Was there enough tubal length? Despite the fact that the tube was burned all the way to the uterus, we were able to establish a beautiful ampullary-cornual reconnection. She had one two-inch-long tube that had no difficulty picking up the egg.
With confidence, we then suggested that Bert also go through vasectomy reversal surgery. Three months later, despite the dire predictions given by her regular doctors, Wanda became pregnant. In most of the cases we have seen where both the man and the woman had previously been sterilized in an earlier marriage, reversing the sterilization on both of them resulted in pregnancy. A more conventional approach for couples in which both the man and the woman have had a sterilization procedure is to perform ICSI on the wife’s eggs using sperm retrieved from the husband’s testicles or epididymis, rather than putting them both through a sterilization-reversal procedure. But I would disagree with that conventional view. I believe the argument still applies that if their sterility could be reversed with minimally invasive surgery, those couples would prefer getting pregnant naturally to undergoing possibly multiple cycles of IVF.
Some doctors have a negative view about women who change their minds and decide they want to have a sterilization reversed. This merely reflects a chauvinistic male attitude that does not admit to the vicissitudes of unpredictable problems that life presents. If your doctor takes that attitude when you ask about sterilization reversal, you might want to consider another doctor.
If you have any questions, you may call us at (314) 576-1400.
Copyright © 2007 by Dr. Sherman J. Silber, M.D.
To purchase how to Get Pregnant by Dr. Silber, Click here