


What Causes PCOS, And How To Treat It?
PCOS, an abbreviation for polycystic ovary syndrome, is a very common cause of infertility in young women, but surprisingly is poorly understood by many infertility doctors. It is characterized by irregular periods (but not always), and infertility with either no ovulation or late ovulation of poor quality eggs. It seems to mystify many doctors and is often referred to as “metabolic syndrome”, indicating their lack of understanding its utter simplicity.
Featured Videos








PCOS is often associated with skin problems ( like oily skin or acne ), or even facial hair above the lips. This is caused by a slightly elevated testosterone and LH/FSH ratio caused by the lack of ovulation. However neither that nor obesity ( as often incorrectly thought of as the cause ) is the cause of PCOS. Those symptoms, along with lack of good ovulation, are simply CAUSED BY THE PCOS. So what causes PCOS?
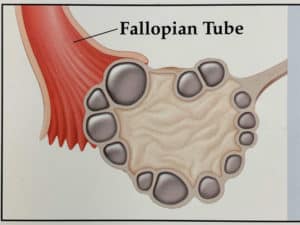
Ironically it is the result of your being born with TOO MANY EGGS. That sounds strange at first. How can too many eggs cause infertility? Women who have an excessive number of eggs in their ovary inhibit the otherwise rapid rise of FSH that should occur on the first day of each menstrual period. Normally the rapid rise of FSH on day 1 of your period recruits a dominant follicle that eventually (out of 1000 eggs every month) will be the one to mature first and the one to ovulate on day 13 or 14. But this rapid rise of FSH on day 1 of your cycle cannot happen if you have “too many eggs”. Once you understand this simple origin of PCOS, it is no longer such an enigma, and the proper treatment is clear.
You can make FSH rise early in your cycle, with either FSH injections or pills like clomid. But that alone is not enough, for several reasons. Firstly, because you have such a huge number of eggs, you might have multiple ovulations and thereby have a dangerous multiple pregnancy. Secondly, the stimulation will impede the proper timing of your uterine lining, preventing the embryo from implanting. That is why the pregnancy rate is so low with ovarian stimulation and IUI (intra-uterine insemination ), a pretty stupid though popular treatment.
So the correct and simplest treatment for PCOS is IVF ( in vitro fertilization). With IVF, we can put back into your uterus just one or two embryos, and safely freeze all the rest for later. So you don’t risk having triplets or more ( which would be very dangerous ). Furthermore we can freeze all the embryos, and put the embryos into your uterus only when the uterine lining is perfectly timed to accept your embryo.
But your next question about PCOS should go beyond merely getting pregnant and having a baby, but rather you should address the whole woman’s health issue of PCOS. Your cycles are irregular and estrogen dominant, causing not only inconvenience at present, but also in the future 20 years from now a higher risk of uterine cancer and heart disease. So to prevent these later complications of PCOS occurring later in your life, you need to turn off this churning out from your ovaries of excessive testosterone. That can be accomplished simply by going on mild birth control pills, 21 days on and 7 days off.
So with PCOS, you should do mini-ivf when you wish to get pregnant, and cyclic birth control pills when you don’t wish to become pregnant. By age 40 you will have lost so many eggs by virtue of getting older, that by then your cycles will become regular and you will no longer need the birth control pills. But you should not wait to 40 to have a baby, because by then your eggs will not be as fertile.
There is an important caveat regarding stupid, incorrect treatment of polycystic ovary syndrome. For some reason, doctors have been fooled by drug company sales people that PCOS, or “metabolic syndrome”, is a mild or early version of diabetes. Nothing could be farther from the truth. But nonetheless most doctors will suggest you go on a pill normally used for type 2 diabetes, METFORMIN. This pill causes glucose and potassium to go intra-cellular, and can delay a diabetic from having to go on insulin. But the side effects are terrible, and it in no way will help the PCOS. We see women with infertility being stupidly put on metformin for years, and never getting pregnant, because metformin simply does not help PCOS at all. Doctors who blindly prescribe metformin to their infertility patients, simply do not understand PCOS, or even in fact, diabetes. Furthermore, by freezing your embryos for a later date we can completely 100% avoid the risk of any dangerous hyperstimulation.
It is often erroneously thought that being overweight causes PCOS. Yet the vast majority of PCOS patients are not at all overweight. PCOS is not caused by overweight or diabetes. It is simply caused by TOO MANY EGGS. And it is easy to treat, getting a very high pregnancy and baby rate, if you understand it’s great simplicity.
Emergence of the Dominant Single Follicle During a Normal Ovulatory Monthly Cycle
At the time of your menses (menstruation), as a result of the rapid fall in estradiol (estrogen) and progesterone secretion from the ovulated follicle of the previous month, the uterus sheds the lining that had built up during that month in preparation for pregnancy. This sudden drop in estrogen causes the FSH secreted from the pituitary gland to rise dramatically around day twenty-six of the previous twenty-eight day cycle. So, two days later, on day one of your menstruation (the beginning of your next cycle), this elevated FSH stimulates only the development of follicles that had left the resting pool four months earlier, and that are now antral. As these antral follicles grow in response to FSH, they secrete estrogen and inhibin B, which in turn suppress further the pituitary secretion of FSH. Thus, as the antral follicles become more mature (by day six), the FSH begins to decline. If these antral follicles were not rescued by the increased FSH level on day one of the menstrual cycle, when they have finally reached the antral size, they would die immediately.
A competitive struggle then ensues between all of these approximately thirty antral follicles to see which one will become the “lead follicle” that will ovulate on day fourteen. The antral follicle that is most sensitive to FSH in the first few days of your cycle becomes even more sensitized to FSH, and thus gains the lead over all the other follicles (which die off because of lower and lower levels of FSH). Once the dominant follicle gains the lead, it will never relinquish it, because it requires less FSH than the others to get the same degree of stimulation. Because FSH continually declines toward the middle of your cycle just prior to your ovulation, all the other antral follicles that month (which have finally become hormone-dependent after almost three months of non-hormone-related growth) will die. When they reach this stage of development, the follicles are completely dependent on FSH for survival. Once the estrogen production exponentially peaks, around day twelve or thirteen, it stimulates a dramatic rise in LH from the pituitary gland, and that rise in LH is what prepares the one remaining follicle for ovulation. It is not just ovulation, but the concurrent maturation of the egg that counts.
In preparation for IVF, FSH injections are given in the early part of the cycle so that the FSH level never declines, as it would normally. This sustained elevation of FSH, which is all that the administration of ovulatory stimulation hormones amounts to, sustains almost all of the thirty or so antral follicles so that no single follicle can gain dominance over the others. Therefore, the number of eggs retrieved in a hormonal stimulation cycle for IVF is directly reflective of your antral follicle count, and your antral follicle count is directly reflective of your total remaining number of eggs.
Note that with our particular stimulation polycystic ovary syndrome protocol, you will not get sick, and therefore will have a much higher pregnancy rate per egg.