


Genetic Testing of Embryos
Genetic testing of IVF embryos before placing them back into the patient can be confusing to the layman, and in the past was often an unnecessary extra expense that was even often in error. However now, in many cases it is of great value to the patient in assuring the healthy baby they want.
We were among the first to do accurate genetic testing of embryos, and our first paper on it appears in the prestigious journal JAMA in 1995. By doing this first case, we prevented a couple from having a baby with cystic fibrosis even though they were both genetic carriers of this disease.
But most patients are not carriers of mutations for a specific genetic disease like cystic fibrosis. Nonetheless some can still benefit from a more general type of genetic testing of embryos. You will have an option to discuss whether genetic testing of embryos is right for you.
Gender Priority
Genetic Testing for Gender Selection
Often couples have already had many children of just one gender, either all boys or all girls. They would like to balance their family or families with the other gender. Some prefer the next child to be a boy, and some prefer the next child to be a girl. We can accomplish this quite simply by doing a safe biopsy of the embryo at blastocyst stage and determine if it is a boy or a girl. We will counsel you on this, and in most cases make it available to you if you wish.
PGT-M Genetic Testing
Video of an Embryo Biopsy
Click on the images below to see the figure illustrations.
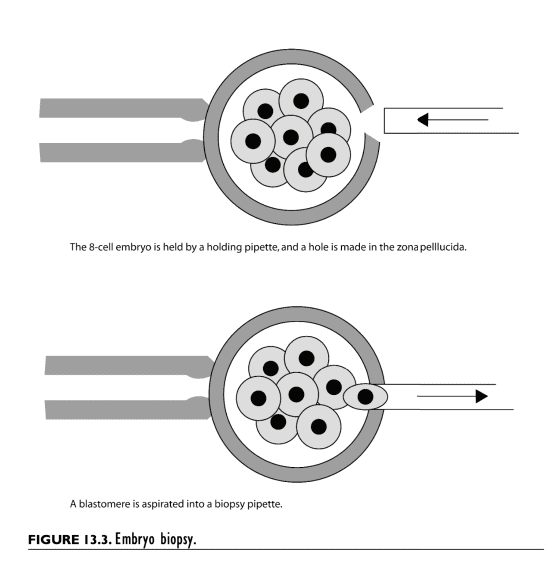
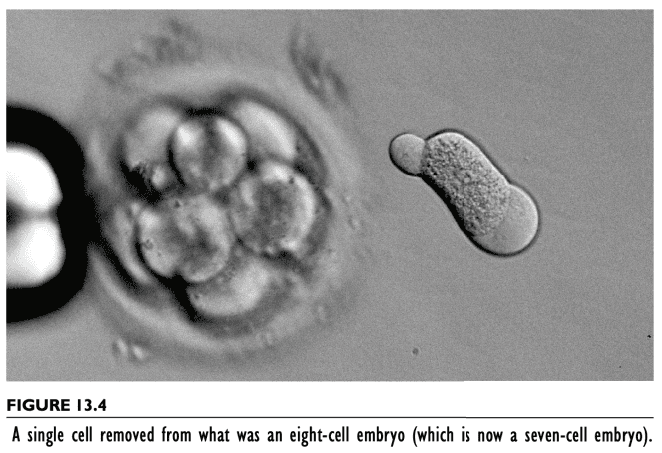
Five cells are removed from a hundred and thirty cell blastocyst (day five)
PGT-M: Genetic Testing for Carriers of Disease
We were among the earliest to test embryos genetically. We published our first such case in JAMA (Journal of the American Medical Association) in 1995. It involved a couple we were treating who had no sperm in his ejaculate because of congenital absence of the vas deferens caused by a mutation in his cystic fibrosis gene. His wife had the same mutation in her cystic fibrosis gene. This meant we had to microsurgically remove sperm from his epididymis (MESA) to fertilize his wife’s eggs, but that 25 per cent of those resulting embryos would be a child with cystic fibrosis. So we genetically tested all the embryos for the cystic fibrosis mutation, and only transferred to her the one without cystic fibrosis, and so she gave birth to a normal baby without the disease that she and her husband both carried. We can do this now for virtually any rare mutation the couple may carry that would otherwise cause some terrible genetic disease in the infant.
These genetic diseases are classified into “autosomal recessive” OR “autosomal dominant”. With autosomal dominant disease mutations, the parent actually has the disease because you need only one copy of a dominant mutation to cause the disease, like Huntington or Marfan disease. We would only transfer to the patient the embryos that do NOT have this one mutation. With autosomal recessive, either or both parents can be carriers of one copy of this mutation and not have the disease. But if their child gets a recessive mutation from each parent and therefore has two copies, he or she will have the disease. There are probably 10,000 terrible autosomal mutations like this. But they are all different. So it is rare for both parents to have a copy of the same rare disease mutation. However if they do, PGT-M solves the problem for them by selecting only the embryos that do not have two copies of the mutation.
SUMMARY PGT-M GENETIC TESTING:
No matter how rare the mutation, if there is any genetic disease or carrier state in the family, we can make sure that the couple’s baby will not have that genetic disease. This genetic testing is extremely reliable. It is called “PGT-M”, which means pre implantation genetic testing for a disease causing MUTATION. It is very successful, although not very commonly needed.
PGT-A Genetic Testing
Click on the images below to see the figure illustrations.

PGT-A: Genetic Testing For Chromosome Abnormality
This is the most common “genetic testing” that is performed in IVF labs. It is very useful and reassuring for certain patients. In the past, PGT-A lowered the success rate rather than increasing it, and resulted in embryos that would have been normal babies being discarded because of an incorrect diagnosis of “abnormal” or “aneuploid”. Furthermore, embryos diagnosed as euploid, or normal, often do not result in a baby. So in the past, PGT-A was problematic.
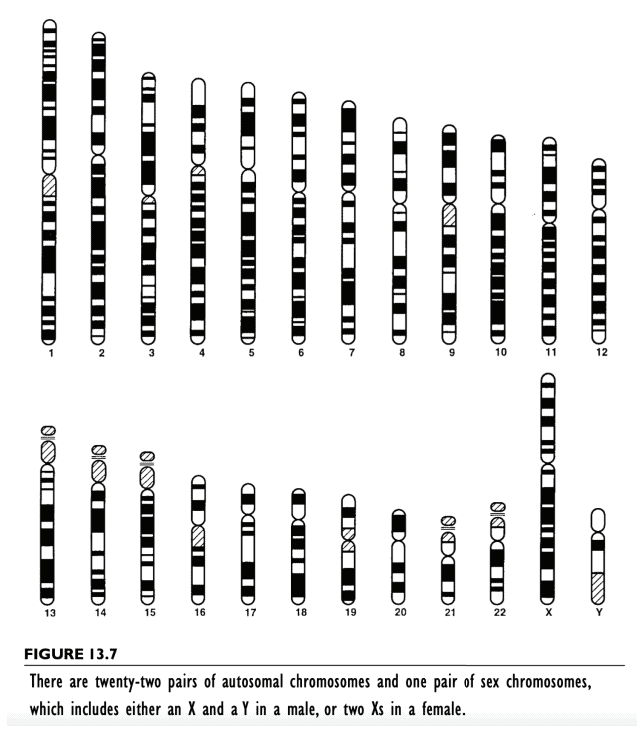
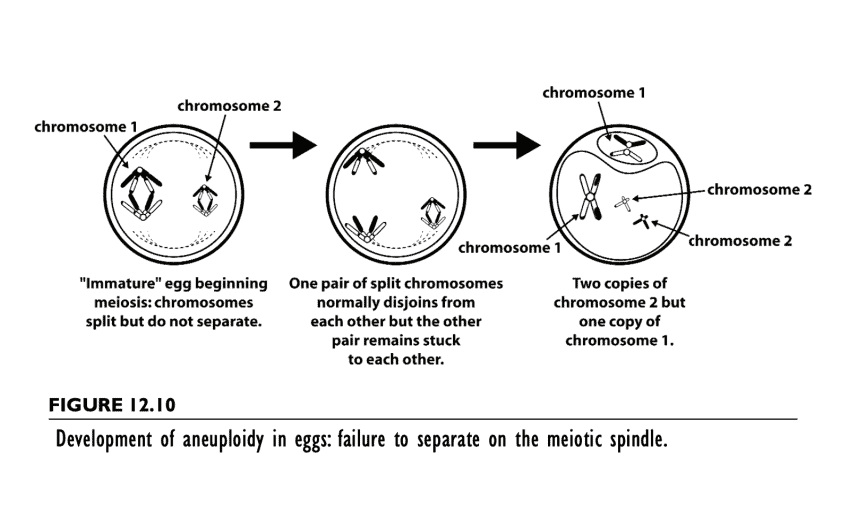
However just very recently, with NGS sequencing, and the diagnosing of “mosaics” correctly (not just calling “mosaics” aneuploid), PGT-A testing now can be very useful and reassuring for certain groups of patients. Let me explain. All we are doing with PGT-A testing is counting chromosomes. You have 46 chromosomes in all of your cells, 23 sets of two. There are 22 autosomes, and 2 sex chromosomes. The female has two X sex chromosomes and the male has a Y and an X. All that PGT-A is doing is counting these chromosomes.
It is not true overall “genetic testing” to make sure the baby is “normal”. There are 23,000 genes and they only represent 2 percent of your DNA. So we are far from being able to test your whole genome. With PGT-A we are just testing to see if the cells in the embryo have the normal number of 46 chromosomes, e.g., if they are “euploid” rather than “aneuploid”.
But the early blastocyst embryo usually has a combination of euploid and aneuploid cells. Eventually those euploid cells outgrow the aneuploid ones a trillion times over. But in the early embryo there is often a “mosaic” of euploid and aneuploid cells. So we now know that it is safe to transfer “mosaic” embryos that used to be diagnosed as “aneuploid”, because many normal embryos at an early time in their development were indeed mosaic when biopsied. That is they had a variety of euploid and aneuploid cells at the time of biopsy. In fact for all of us “normal” adults, out of 50,000 cells tested there will be a few aneuploid cells left over from this early embryonic period of our fetal lives. Also since aneuploidy or euploidy is only one small part of embryo development, embryos diagnosed as “euploid” often lead to no pregnancy anyway, or to miscarriage, despite the patient being told they are normal.
So what is the benefit of PGT-A “genetic” testing today? To whom should we offer it? It has two strong benefits to women between ages 34 and 40. The embryos that are diagnosed now with NGS as “aneuploid” truly are “aneuploid”. We can be sure they will NOT result in a successful pregnancy. Those diagnosed as “mosaic” or “euploid” are not aneuploid, and could result in a successful pregnancy.
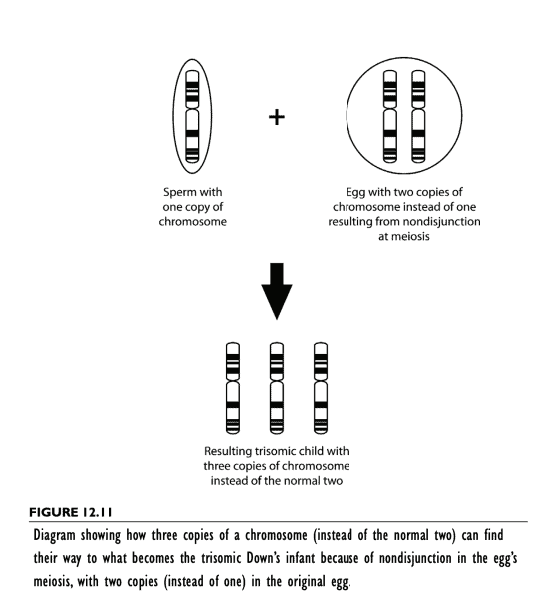
So the benefits for some patients would be limited. For others the benefits would be very appealing. The risk of Down syndrome in 35 year olds is about one in 500, very low. But by age 40 the risk is 1%. This is still extremely low. But for many couples it is terrifying. PGT-A will virtually eliminate the risk of Downs. Also it will reduce (not eliminate) the risk of miscarriage. So PGT-A seems most appealing from ages 34-40.
PGT for Translocation
Click on the images below to see the figure illustrations.
Preimplantation Genetic Testing (PGT) for Translocations
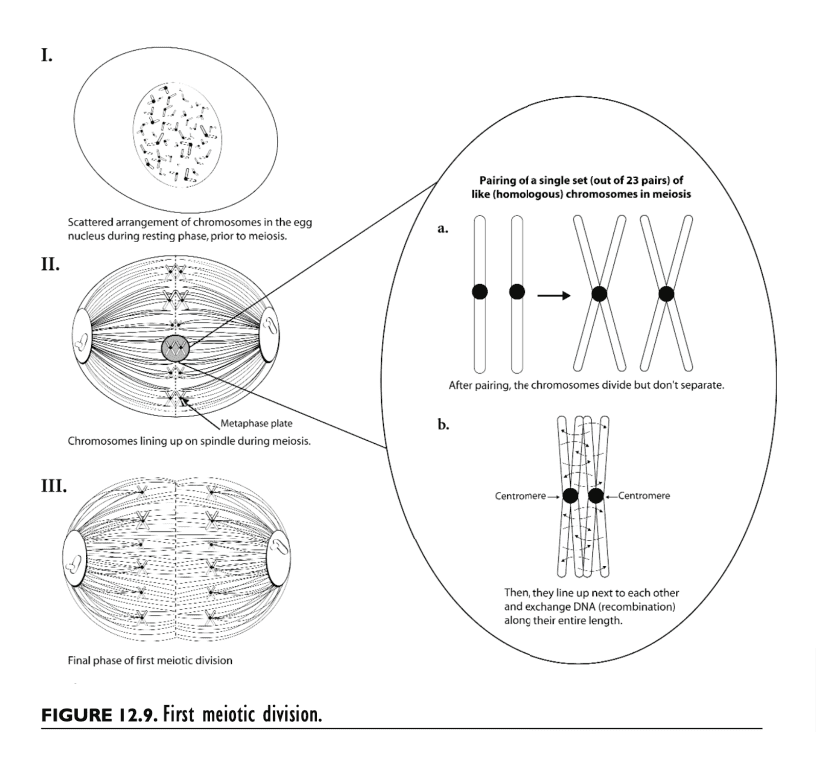
About 2% of miscarriages are caused by a “translocation”. This means that both parents have all their genes. Nothing is missing. They are normal. But some of their DNA is located on the wrong chromosome. This poses no problem for their health, but with the rearrangements of chromosomes that occurs in the sperm and the egg at meiosis, the embryo could wind up with a “translocated chromosome” and have too many or two few genes associated with that translocated chromosome. This can cause recurrent miscarriage or just no pregnancy at all. We can prevent miscarriage in such cases by testing for the translocation, and only transferring to the embryos that have either no translocation or a “balanced” translocation like the patients themselves have, but not transfer embryos with an “unbalanced” translocation, that have too many or too few genes.
SUMMARY OF TRANSLOCATION TESTING:
If you have miscarriages, we should get karyotype on both husband and wife to see if there is a balanced translocation causing the miscarriage (2%). We can then test for it and prevent future miscarriages.
PGT-P Genetic Testing
Click on the images below to see the figure illustrations.
PGT-P: Advanced Genetic Testing to Prevent Common Genetic Diseases in Adulthood
PGT-P is more complicated and a bit abstract to try to explain. There is an aphorism in genetics: “Rare diseases like cystic fibrous or muscular dystrophy are caused by common carrier mutations. But common diseases like diabetes or cancer etc are caused by an assortment of rare combinations of rare mutations, that by themselves produce no abnormality.” Thus we know that the risk of a baby growing up and getting diabetes type 1 or high blood pressure or heart disease or cancer are genetic. But with rare exception (like BRCA for certain breast and ovary cancers), we have no idea what is the combination of multiple DNA sequence variants that cause these common diseases.
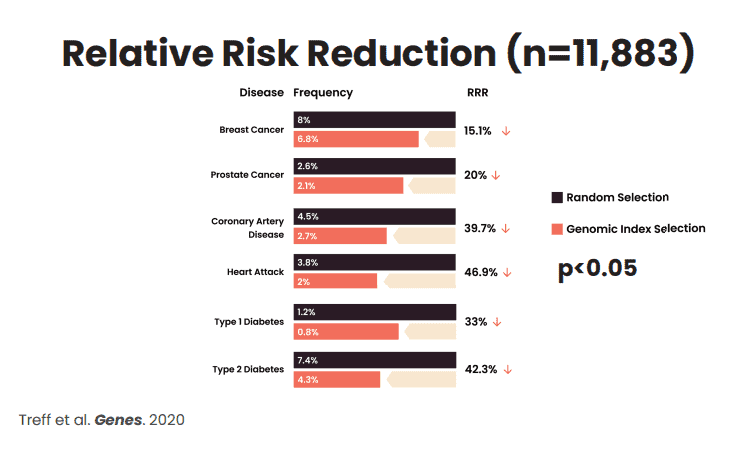
However, now with massive computer power, we can determine a risk factor of an embryo becoming a child with a higher or lower chance of developing one of these common adult diseases, later in life. We can thereby choose to transfer the embryo (s) that are least likely to develop these common diseases, later in life. No guarantee. But it reduces the risk factor for your baby getting one of these terrible diseases as he or she grows up.
View the chart below the video to find out how much PGT-P might reduce your child’s risk of developing such diseases perhaps later in life.